
Safe Baby Sleep Tips Every Parent Must Know reflects dominant search intent around safe sleep for newborn, baby sleep position, back to sleep guidelines, crib safety rules, room sharing without bed sharing, reducing SIDS risk, newborn sleep environment, and safe swaddling practices. Infant sleep safety is not preference based. It is risk mitigation grounded in epidemiology, respiratory physiology, and environmental control. Sudden unexpected infant death is strongly associated with sleep positioning, surface softness, overheating, and airway obstruction. Structured adherence to evidence based sleep principles reduces preventable mortality.
Back Sleeping and SIDS Risk Reduction
Placing infants on their backs for every sleep period is the central intervention in safe sleep guidance. The American Academy of Pediatrics states that supine positioning significantly reduces the risk of sudden infant death syndrome. Back sleeping maintains airway patency and lowers rebreathing of carbon dioxide.
Side and stomach positions increase risk due to potential airway obstruction and impaired arousal response. Prone positioning can cause rebreathing of exhaled air trapped in bedding. Infants lack the neck strength and motor control to reposition consistently.
The “Back to Sleep” campaign, now expanded to “Safe to Sleep,” contributed to substantial reductions in SIDS rates after its introduction. The National Institute of Child Health and Human Development documents measurable declines in sleep related infant deaths following widespread public health education on supine sleep.
Airway Physiology in Supine Position
Concerns about choking while lying on the back are not supported by anatomical evidence. The trachea lies anterior to the esophagus. When supine, regurgitated milk is more likely to pool away from the airway. Infants possess protective gag and cough reflexes.
Consistency Across Sleep Periods
Back positioning must apply to nighttime and daytime naps. Risk accumulates across sleep episodes. Inconsistent positioning undermines protective effect.
Crib Safety and Sleep Environment Control
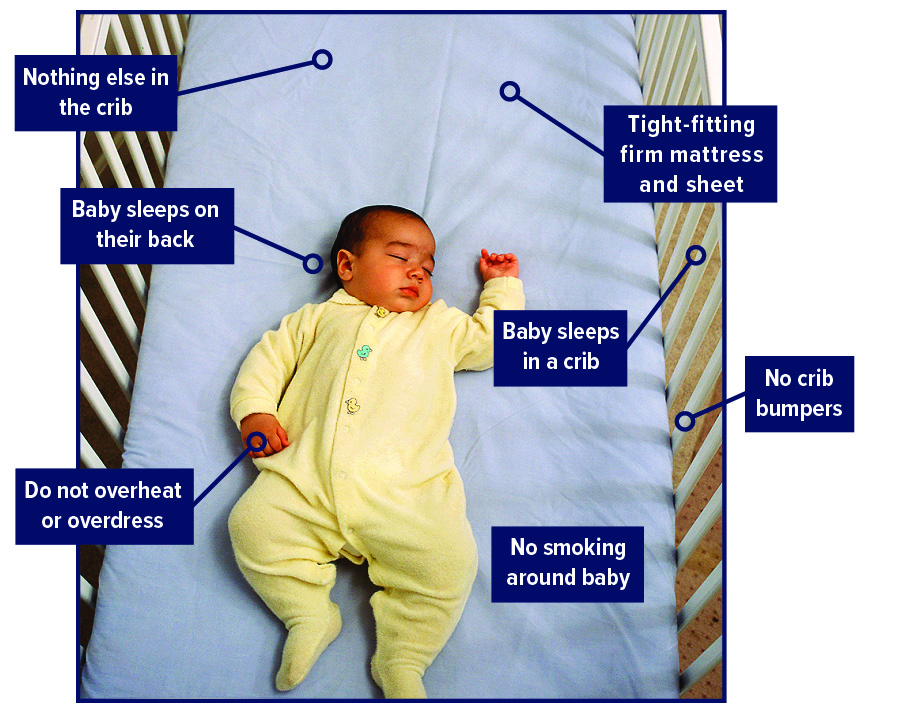
The sleep surface must be firm, flat, and free of soft objects. The Centers for Disease Control and Prevention identifies soft bedding, pillows, loose blankets, and stuffed toys as modifiable risk factors for sleep related infant death.
A safety compliant crib with a tight fitting mattress and fitted sheet is recommended. Crib bumpers are not protective and can create suffocation hazards. The sleep area should remain uncluttered.
Room sharing without bed sharing is advised for at least the first six months. The American Academy of Pediatrics recommends placing the infant’s crib or bassinet in the caregiver’s room but on a separate surface. Bed sharing increases risk due to overlay, entrapment, and soft bedding exposure.
Temperature Regulation
Overheating is associated with increased SIDS risk. Dress the infant in one layer more than an adult would wear in the same environment. Avoid hats during indoor sleep. Maintain a comfortable room temperature.
Sleep sacks are preferable to loose blankets. They provide warmth without covering the face.
Surface Integrity
Sofas and armchairs are unsafe for infant sleep. The risk of entrapment between cushions is significant. Portable sleep devices not designed for routine sleep should not replace a safety certified crib or bassinet.
Safe Baby Sleep Tips for Safe Swaddling and Sleep Positioning
Swaddling can calm newborns but must be applied correctly. Swaddled infants must always be placed on their backs. Once an infant shows signs of rolling, swaddling must stop due to increased suffocation risk.
The National Health Service explains that swaddling should allow hip flexion and movement to prevent hip dysplasia. Tight wrapping around the hips restricts natural joint positioning.
Transition from Swaddling
Rolling typically begins around three to four months, though variation exists. Transition to wearable sleep garments when early rolling attempts appear.
Avoiding Weighted Products
Weighted blankets and sleep products marketed for infants are not supported by safety data. Added weight may impair chest wall movement and breathing.
Feeding, Pacifiers, and Nighttime Care
Safe Baby Sleep Tips recognize that breastfeeding is associated with a reduced risk of sudden infant death syndrome. Within Safe Baby Sleep Tips guidance, data from the Centers for Disease Control and Prevention indicate that longer breastfeeding duration correlates with lower rates of sleep related infant death, potentially due to immune protection and improved arousal regulation.
Safe Baby Sleep Tips also include offering a pacifier at sleep time once breastfeeding is firmly established. Under Safe Baby Sleep Tips recommendations, the American Academy of Pediatrics supports pacifier use during naps and bedtime as a measure that may further reduce sudden infant death risk.
Night Feeding Safety
Caregivers must avoid falling asleep with infants on couches or armchairs during feeding. If bed sharing occurs unintentionally, return the infant to a separate sleep surface immediately after feeding.
Smoke Free Environment
Prenatal and postnatal smoke exposure significantly increases SIDS risk. The World Health Organization outlines the harmful respiratory effects of tobacco exposure on infants. Maintain a smoke free home and car.
Developmental Milestones and Sleep Adjustments
As infants grow, sleep patterns evolve. Rolling, sitting, and crawling change risk dynamics. Once infants can independently roll from back to stomach and stomach to back, they may choose their own position. Continue placing them on their back initially.
Crib mattress height should lower as the infant gains mobility to prevent falls. Remove hanging toys within reach.
Monitoring Devices and False Security
Commercial sleep positioners and home cardiorespiratory monitors are marketed as safety tools. However, the American Academy of Pediatrics states that there is no evidence these devices reduce SIDS risk in healthy infants. Reliance on unproven technology can create false reassurance.
Travel and Alternative Sleep Settings
When traveling, ensure access to a firm flat sleep surface. Portable cribs meeting safety standards are appropriate. Avoid improvised sleep spaces such as adult beds or soft cushions.
Epidemiology of Sleep Related Infant Death

Sudden unexpected infant death includes SIDS, accidental suffocation, and undetermined causes. Risk peaks between one and four months of age. Multifactorial interaction between vulnerable infant, critical developmental period, and external stressors defines the triple risk model.
Public health campaigns emphasizing supine sleep, firm surfaces, and smoke free environments correlate with significant mortality reduction. However, disparities persist across socioeconomic and demographic groups.
Addressing structural factors such as access to safe sleep spaces and caregiver education improves compliance.
Physiological Basis of Arousal and Airway Control
Infants possess immature autonomic regulation. Arousal response to hypoxia may be blunted in vulnerable infants. Prone positioning can impair heat dissipation and increase carbon dioxide rebreathing.
Firm surfaces reduce facial indentation and airway obstruction. Soft bedding conforms around the face, trapping exhaled carbon dioxide.
Cultural Practices and Risk Evaluation
Bed sharing practices vary globally. Risk increases when combined with soft bedding, parental smoking, alcohol use, or extreme fatigue. Risk analysis must consider cumulative factors rather than single behaviors.
Education must focus on modifiable hazards. Blanket prohibition without contextual understanding reduces adherence.
Structured Implementation Framework
- Always place infant on back for sleep.
- Use firm flat surface with fitted sheet only.
- Keep crib free of soft objects.
- Share room, not bed, for first six months or longer if feasible.
- Maintain smoke free environment.
- Regulate temperature and avoid overheating.
- Discontinue swaddling at first sign of rolling.
Safe Baby Sleep Tips Every Parent Must Know are operational principles grounded in epidemiological data and infant physiology. Risk reduction depends on consistent implementation across every sleep episode. Infant sleep safety is cumulative. Each controlled variable decreases probability of preventable harm.